Stroke medicine
We have written this leaflet to tell you more about mechanical thrombectomy for treatment of an ischaemic stroke, including the benefits, risks and what you can expect when you have this procedure.
What is ischaemic stroke?
An ischaemic stroke occurs when an artery (blood vessel) is blocked by a clot, cutting off the blood and oxygen supply to that part of the brain. Without blood supply, brain cells lose function and eventually die.
What is mechanical thrombectomy (clot retrieval)
Thrombectomy is an emergency procedure performed by a specialist team led by a doctor called an Interventional Neuroradiologist. The doctor uses specialised equipment and guidewires to physically remove the clot from the artery in the brain in order to restore the supply of blood.
What is thrombolysis?
Some patients will have thrombolysis in conjunction with thrombectomy if the clot is blocking a major vessel in the brain. Thrombolysis is a treatment that uses a strong “clot busting” medication, known as a thrombolytic agent, which is given through a needle in the vein (cannula), to try and dissolve the clot blocking the supply of blood.
Thrombolysis is a time critical treatment and must be given as soon as possible after onset of symptoms of acute ischaemic stroke to maximise the benefits of treatment. It is usually only given within 3 to 4.5 hours after onset. Thrombolysis is not without risk and is not suitable for every patient, including those who are at higher risk of bleeding (for example, those who take anticoagulants such as Warfarin, Apixaban, Rivaroxaban etc.).
If thrombolysis is not feasible (bleeding risk etc.) then mechanical thrombectomy alone may be considered.
What happens during mechanical thrombectomy?

- An incision into an artery in the groin is made and the thin plastic tube (and guidewire is inserted).
- An X-ray detectable dye is injected to highlight the blood vessels which supply up to and into the brain.
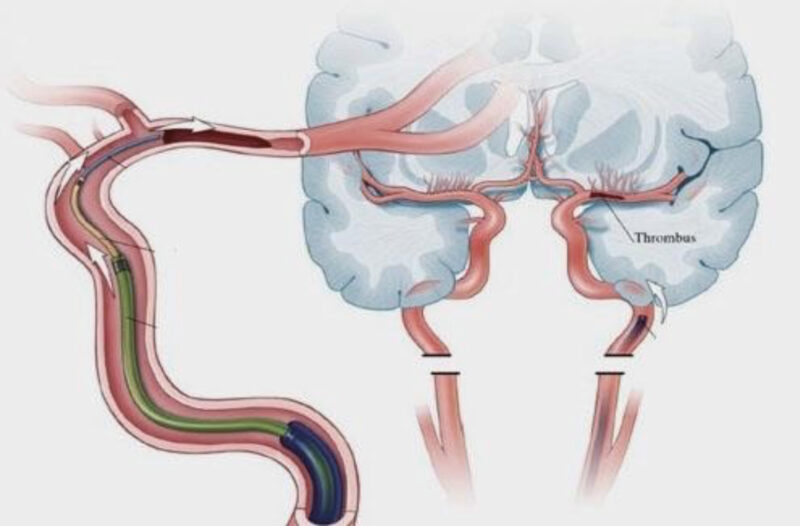
- An X-ray scanner then monitors the highlighted blood vessels and helps guide the route of the catheter up to the brain, and towards the artery which is blocked by the blood clot.
- Once the blockage is reached, a clot-removal device is placed through the catheter tube to take the clot out. We use special equipment such as a small wire mesh (stent retriever) or suction devices to remove the blood clot and re-establish blood flow to the affected part of the brain.
The procedure opens the artery in about 70% of cases. Occasionally, it may not be possible to get to the clot or remove.
What are the benefits of mechanical thrombectomy?
Undergoing this procedure gives around 45% chance of regaining independence. The sooner it is performed the better the chance of recovery, including greater chance of improving current stroke symptoms.
The longer the clot blocks the blood supply in the brain, the more damage will occur and therefore not every patient will completely recover. More than 40% of patients who undergo thrombectomy will benefit (less disability) over those who do not have the procedure.
What are the risks of mechanical thrombectomy?
As with any procedure, there are risks associated with thrombectomy, but overall the potential benefits outweigh the potential risks.
- The contrast dye carries a small risk of allergic reaction, and although rare, can affect the kidney function, this is usually only temporarily (less than 5%, unless you have predisposing risk factors).
- There is a risk related to the groin puncture site, this includes bruising, swelling, infection or bleeding in the groin (7%). In very rare cases people need surgery to repair the artery in the groin to prevent the circulation to the leg being affected (less than 3%).
- There is a risk of bleeding in the brain which can lead to disability or death (5%).
- There is a very small risk of tearing the artery (less than 1%) or re-blockage of the artery, which may lead to disability or death (less than 3%).
- There is a very small risk (less than 5%) that the brain may swell and make further surgery necessary.
What happens after mechanical thrombectomy care?
The nurses will check your observations such as blood pressure, heart rate, oxygen levels, conscious level, checking your groin and the pulses in your feet usually for a minimum of 24 hours.
You will need to remain on bedrest for four hours after the procedure. This will help prevent any complications to the groin. Intermittent compression stockings are usually applied to help prevent clots forming in the legs (deep vein thrombosis) whilst you are in hospital and less mobile.
You will have a repeat CT head scan after 24 hours to rule out any post procedure complications. If there has been no bleeding within your brain, then you will be started on Aspirin or similar medications to reduce the risk of any further blood clots.
When will I be transferred back to my local hospital?
You will be transferred back to your local stroke unit by an ambulance. The transfers usually happen either on the same day, or on the day following the procedure. However, some patients may need ongoing monitoring at the comprehensive stroke centre for a longer period.
Once back at your local stroke unit, you will receive ongoing stroke rehabilitation and follow up in the hospital nearer to your home.
Further information
Contact details
We hope this information sheet has been helpful to you, but it is by no means a replacement for talking to a member of the stroke team. Please ask questions if you feel that you need more information. Alternatively, call the stroke unit on 01642 854534 at any time, we are available 24 hours a day, 7 days a week.
NHS Choices
- Telephone: 111 (when it is less urgent than 999). Calls to this number are free from landlines and mobile phones.
- You can also access us via our website at: www.nhs.uk
Useful websites
- If you would like to find accessibility information for our hospitals, please visit
www.accessable.co.uk - The Stroke Association also has useful information on their website at www.stroke.org.uk
Contact us
If you require further information please contact the stroke team on:
Telephone: 01642 854534
Email: tbc
Patient experience
South Tees Hospitals NHS Foundation Trust would like your feedback. If you wish to share your experience about your care and treatment or on behalf of a patient, please contact The Patient Experience Department who will advise you on how best to do this.
This service is based at The James Cook University Hospital but also covers the Friarage Hospital in Northallerton, our community hospitals and community health services.
To ensure we meet your communication needs please inform the Patient Experience Department of any special requirements, for example; braille or large print.
T: 01642 835964
E: [email protected]